Hello Reader! I’m excited to start our rotations in Taiwan. Hopefully you’ll find our blogs helpful and fun to read.
Steven and I started our day rounding with Dr. Chien-Ming Chen, the only physician in Hem/Onc. Steven wrote a lot about what we saw already, so you can refer to his posts. 🙂
Patient 1: Female patient had triple negative breast cancer, which means that the cancer does not express the estrogen receptor, progesterone receptor, or Her2/neu. Monoclonal antibodies used for breast cancer usually target one of the receptors, such as trastuzumab targeting Her2/neu. With triple negative breast cancer, prognosis is usually poor as targeted treatment cannot be used. Treatment options include surgery and chemotherapy.
Dr. Chen mentioned that many times, biopsy results can take up to 3-4 weeks and getting the approval for an expensive drug can take up to a week. This can be frustrating as the therapy is highly effective and results can be seen within 1-2 days. Within that time frame, a patient’s symptoms can worsen, which is very frustrating to the oncologist.
When shadowing Dr. Chen, he often had to tell the family members to prepare and make plans in case the worst happens. He mentioned that doctors have difficulty telling patients bad news, even after many years of practice. It is even harder when the doctor becomes friends with the patient and his or her family.
We finished early on the 1st day, so I went to Nephrology with Felicia in the afternoon.
Patient 2: Dr. Lin and Felicia had already rounded on most of the patients but we made a quick stop to the ICU to see a patient with septic shock and an UTI. She came in initially with abnormal extension posturing.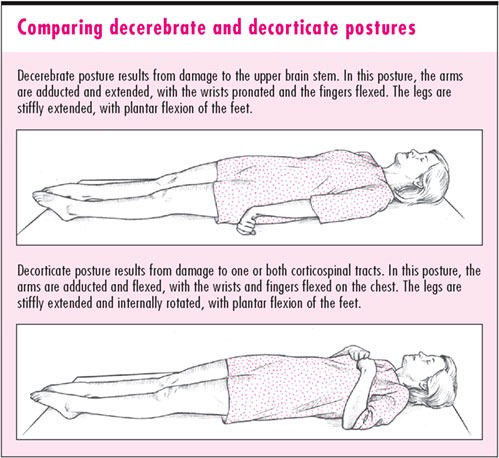
Abnormal extension to pain indicates decerebrate rigidity, which usually indicates brain stem damage below the red nucleus. Posture is an indication for brain damage and is used to determine the severity of a coma with the Glasgow Coma Scale. 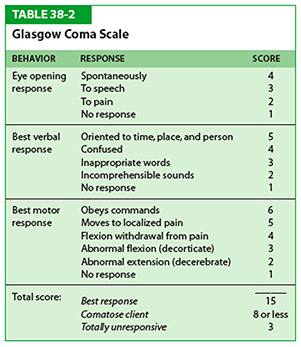
When we saw this patient in the ICU, she wasn’t extended anymore, but was still in pain and confusion. On Day 3 during rounds, we found out that she also had VRE: Vancomycin Resistant Enterococci. Our physician warned us not to touch or get too close to her. With VRE, optimal approach is uncertain but linezolid and quinupristin-dalfopristin are approved for use after susceptibility testing.
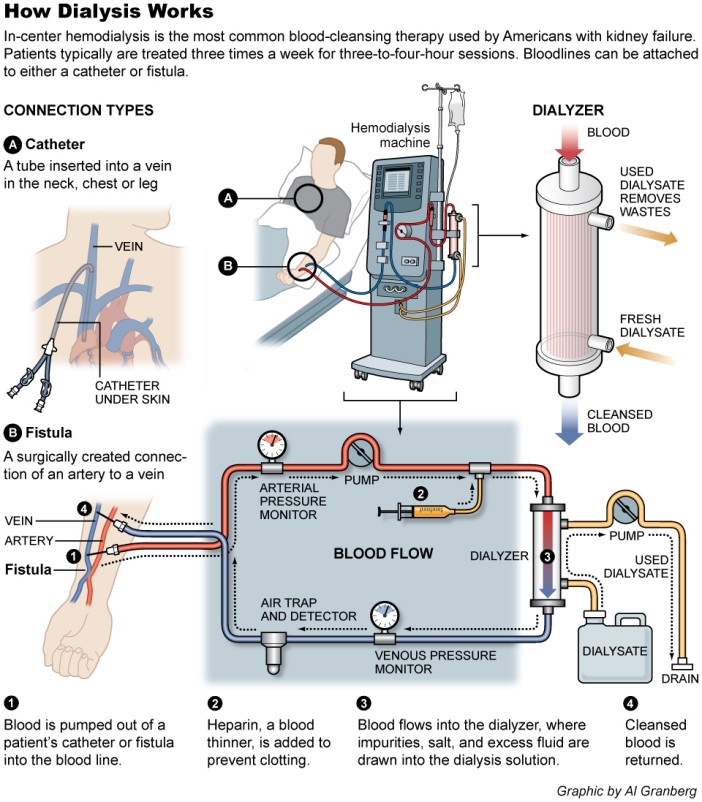
Next, we went to the dialysis department. Patients come in every 2-3 days a week. Monitoring patients is important as dialysis can cause ischemia, hypotension, shock, thrombosis, etc. If there seems to be clots, heparin is used. Low molecular weight heparin is not available in the hospital due to financial reasons. In Taiwan, patients coming in for dialysis usually present with high uremic syndrome or arrhythmias already. The nephrologist explained how the machines work and how they monitor their patients for complications. Interestingly, the machine acts only 10% as effectively as an actually kidney.
Our kidneys do so much work for us! Our nephrologist also mentioned that even current doctors have difficulty managing kidney problems and often refer to him. Makes sense, renal physiology and pathology is tough! I learned a lot the first day. Thanks for reading.
